Product Tour
Every patient.
Every signal.
PeriOptima connects patients and their clinical teams across the full surgical journey: validated risk science, real-time monitoring, and a direct line between patient and clinician that stays open from pre-op through home recovery.
Pre-Surgery
Most complications don't start in the OR. They start weeks earlier, with incomplete data, missed risk signals, and protocols that treat every patient the same. PeriOptima changes that before the patient reaches the operating table.
Risk Stratification
Every validated risk model. One complete view.
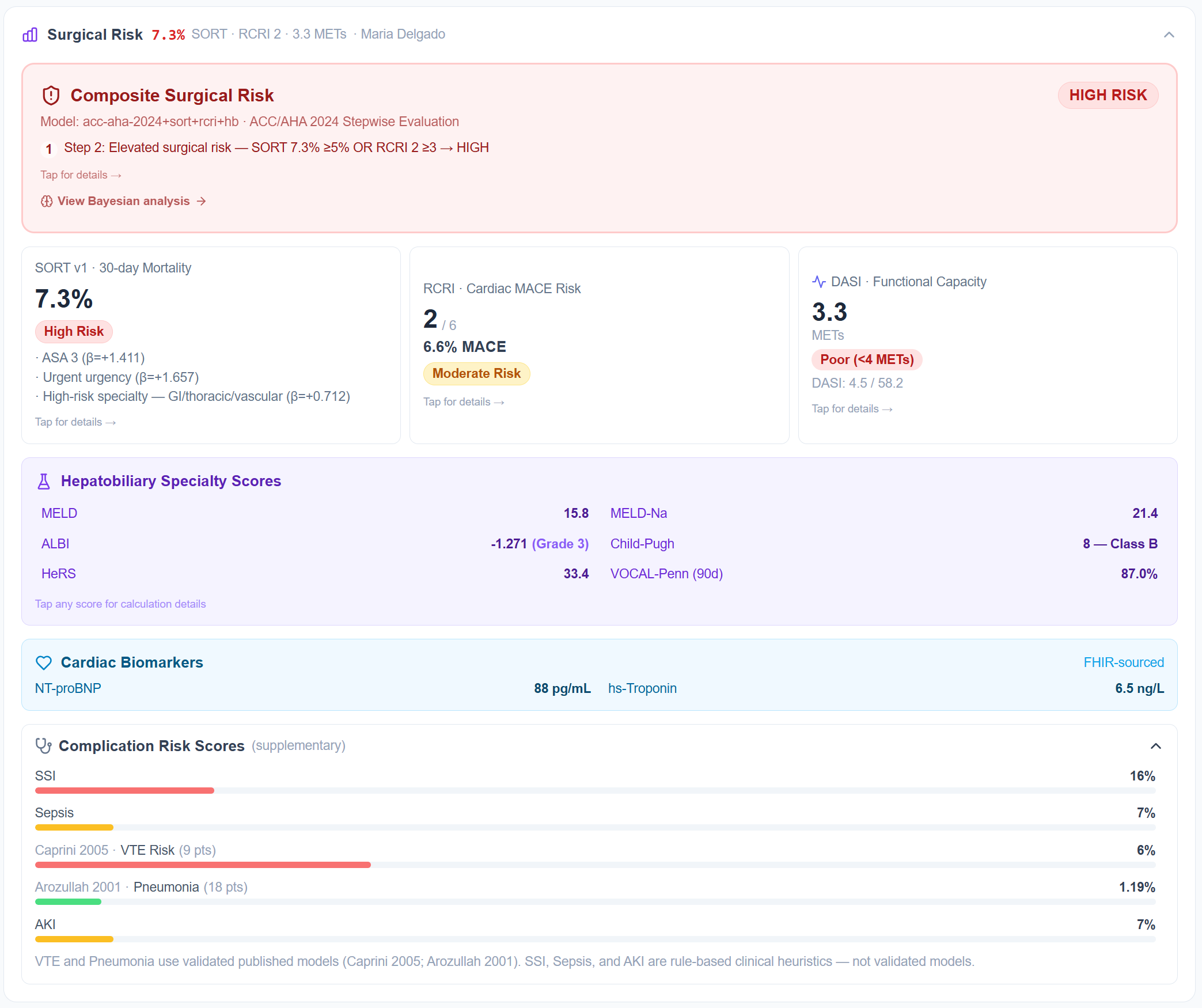
PeriOptima automatically calculates a comprehensive risk profile for each patient using data pulled directly from the EHR via FHIR. SORT v1 for 30-day surgical mortality. RCRI and DASI for cardiac risk and functional capacity. Caprini for VTE. The full hepatobiliary panel (MELD, ALBI, Child-Pugh, VOCAL-Penn) for hepatic surgery patients.
These aren't estimates entered manually. Maria's 7.3% SORT score and high Caprini VTE risk are calculated from her actual clinical record. Risk calculators that used to sit buried in the EMR are now surfaced automatically, before the first appointment.
- SORT v1, validated across 4M+ procedures
- RCRI / DASI, per ACC-AHA 2024 guidelines
- Caprini 2005, standard of care for perioperative VTE
- MELD / Child-Pugh / ALBI / VOCAL-Penn for hepatobiliary populations
Clinical Transparency
Peer-reviewed models. Every input visible.
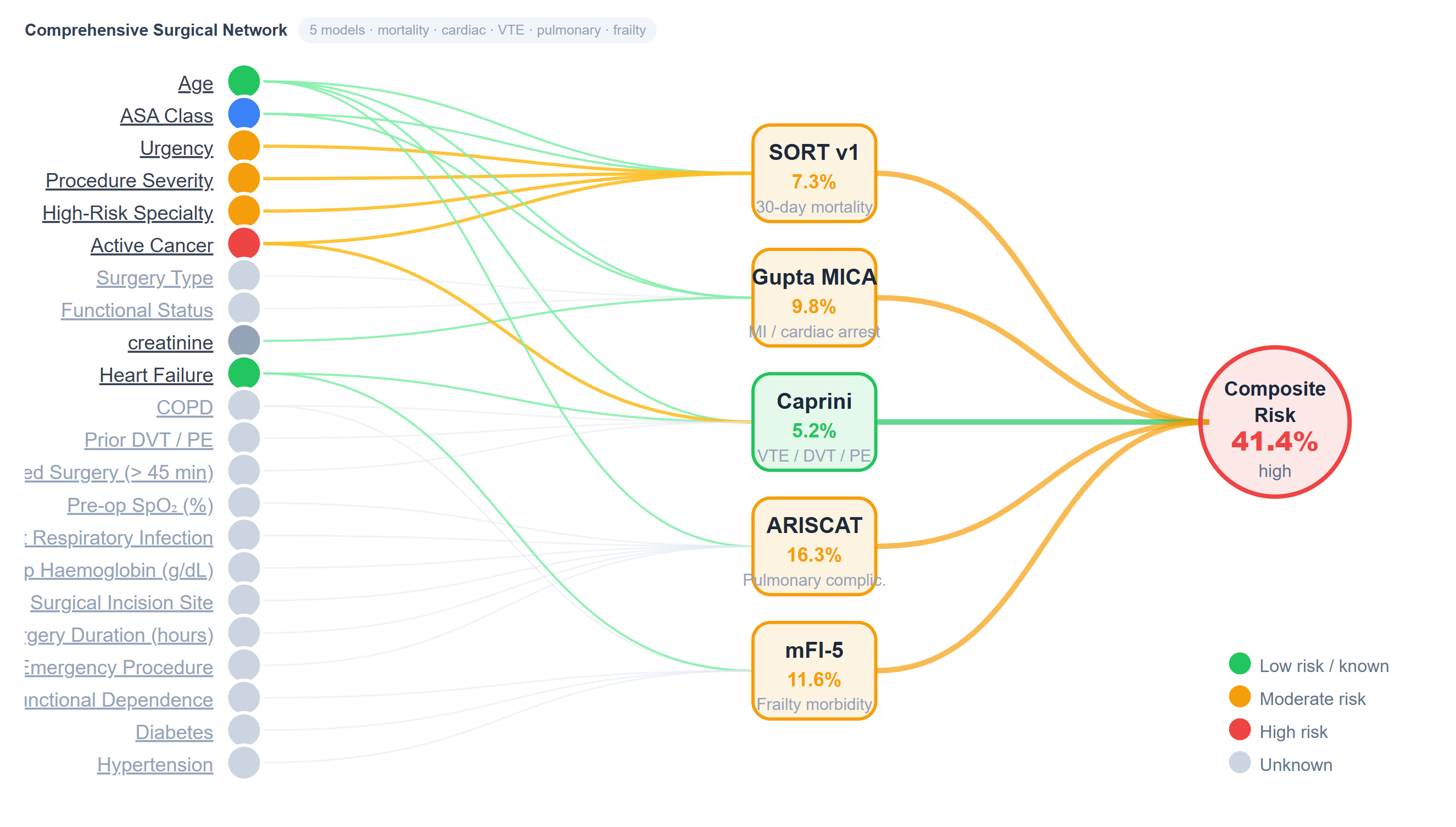
Every risk calculation in PeriOptima traces back to a published, peer-reviewed clinical instrument. The Bayesian risk network shows exactly which patient variables are driving each model's output, down to the individual input and its contribution to the composite risk score.
This isn't a proprietary black box. Clinicians can see why a patient is flagged as high risk, and explain it to the patient, the surgical team, and the anesthesiologist. Validated science. Transparent by design.
Composite Surgical Risk: 41.4%, driven by elevated SORT, Caprini, and ARISCAT scores, each traceable to specific clinical inputs from the patient's EHR record.
Patient Preparation
Maria's prep plan isn't generic. It's hers.
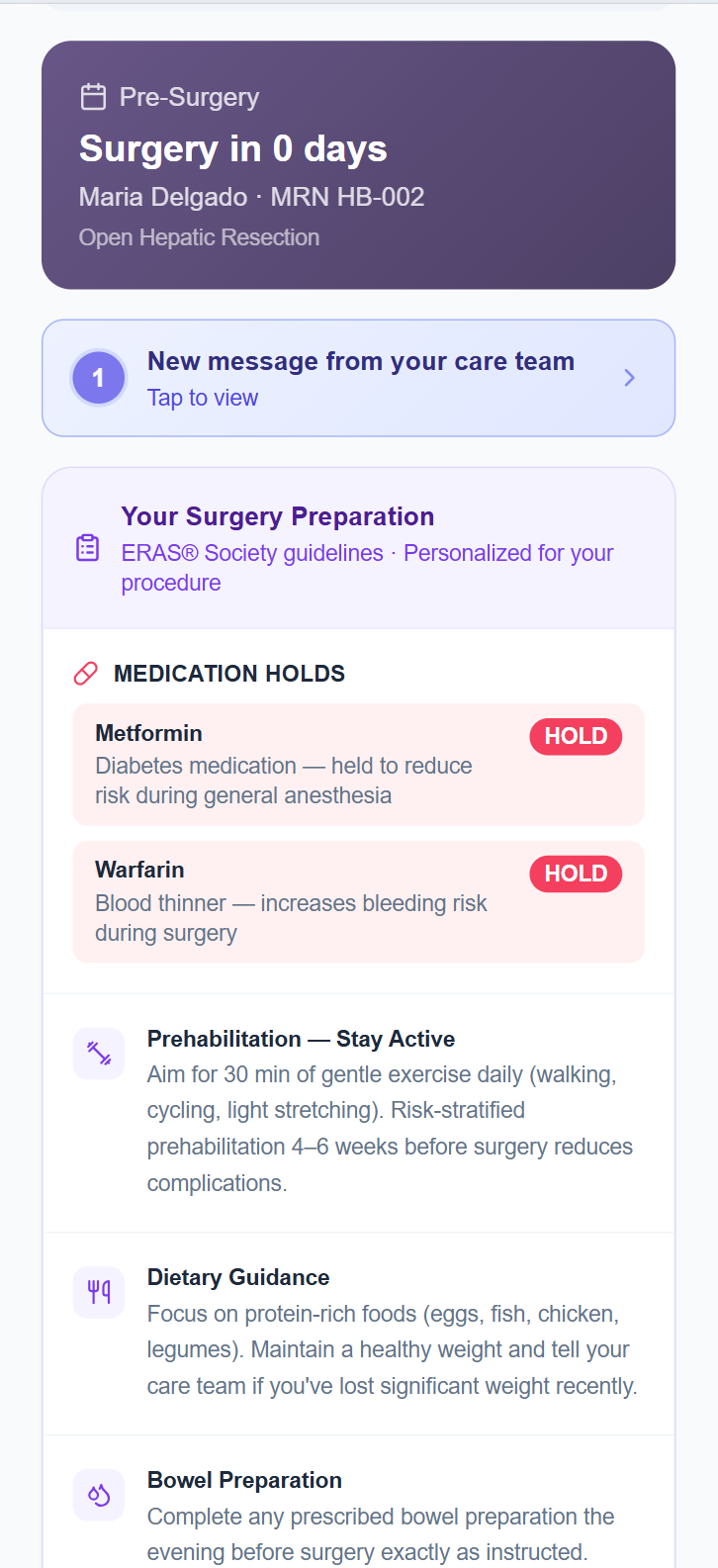
The patient's preparation guidance is built directly from their risk profile. Maria's high Caprini score and documented DVT history triggered a Warfarin hold. Her Metformin was flagged for pause before general anesthesia. Her prehabilitation protocol (30 minutes of daily gentle exercise, 4–6 weeks) reflects her specific procedure and functional capacity score.
All of it delivered to her phone in plain language, updated as her clinical picture changes. Not a generic discharge sheet sent after the pre-op appointment. A living preparation plan, connected to her care team.
- Medication holds flagged from risk scores, not manual review
- ERAS® Society prep guidelines, personalized to procedure
- Prehabilitation targets based on functional capacity assessment
- Direct messaging channel to care team, active before surgery
Patient-Reported Input
The patient's input feeds the clinical model.
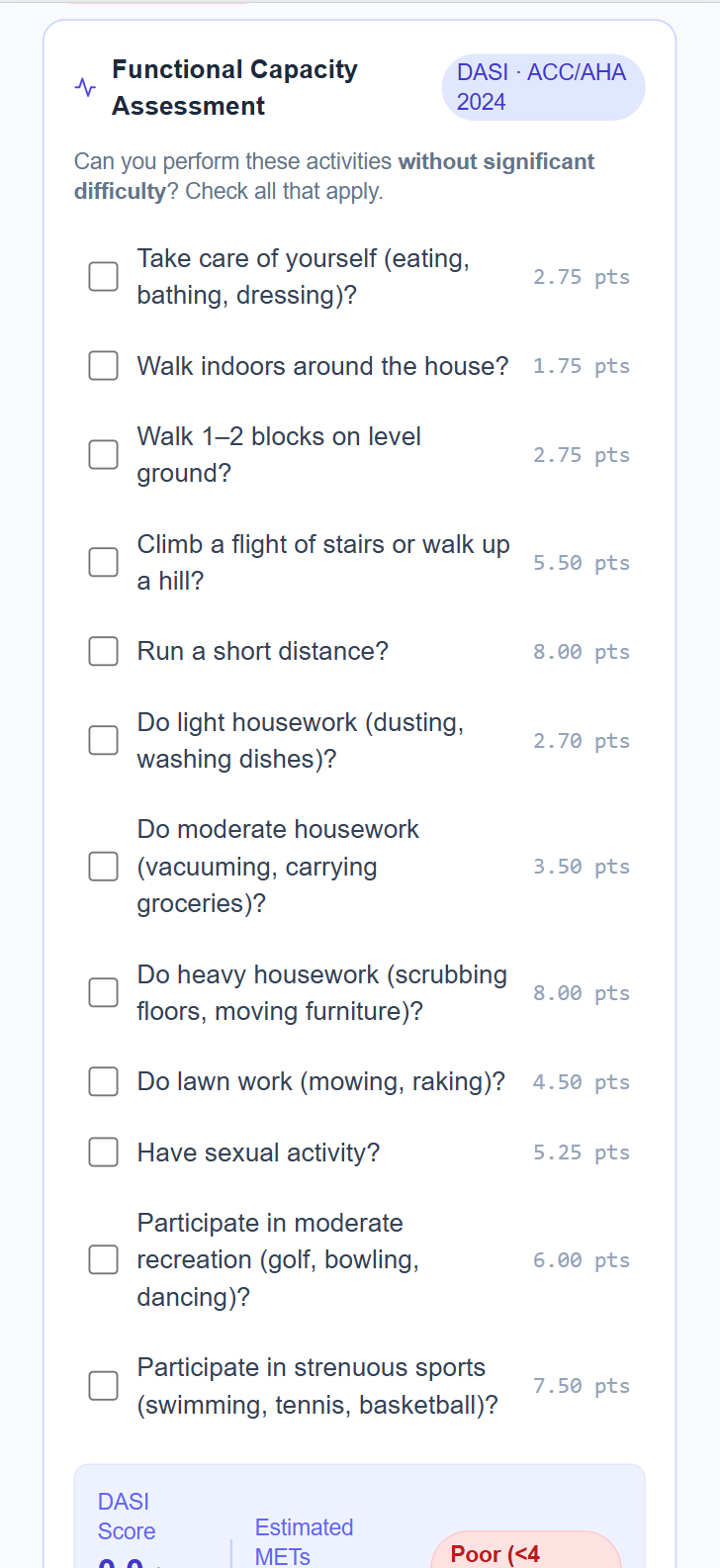
Functional capacity is one of the most important predictors of cardiac risk in surgery, and one of the hardest to assess from EHR data alone. PeriOptima guides the patient through the DASI questionnaire in their app, collecting the activity data that feeds directly into the RCRI/DASI cardiac risk calculation per ACC-AHA 2024 guidelines.
The patient doesn't know they're filling in a clinical instrument. They're answering a question: which of these activities can you do without significant difficulty? Their answers become a METs estimate that updates the composite surgical risk before the pre-op visit.
In Hospital
The most dangerous window in a patient's life starts the moment they enter the OR. Clinical teams need real-time visibility across every patient, without managing a wall of noise. PeriOptima surfaces what matters, when it matters, to the right person.
Clinical Dashboard
Every patient. Every alert. In real time.
The clinical dashboard gives care teams a live summary of their entire patient cohort. 10 active patients enrolled in monitoring. 12 open alerts, 6 of them high priority. SLA compliance for high-alert response at 77.8%, with the system flagging that this is 17 points below the 95% target. Average length of stay at 8 days, one day over benchmark.
The dashboard doesn't just report. It tells the clinical team where the standard of care isn't being met, and makes it impossible to overlook.
- Active patients broken down by status: monitoring, discharged
- Open alert count with high-priority split
- SLA compliance tracking against defined targets
- Average LOS versus procedure benchmarks

Smart Alert Routing
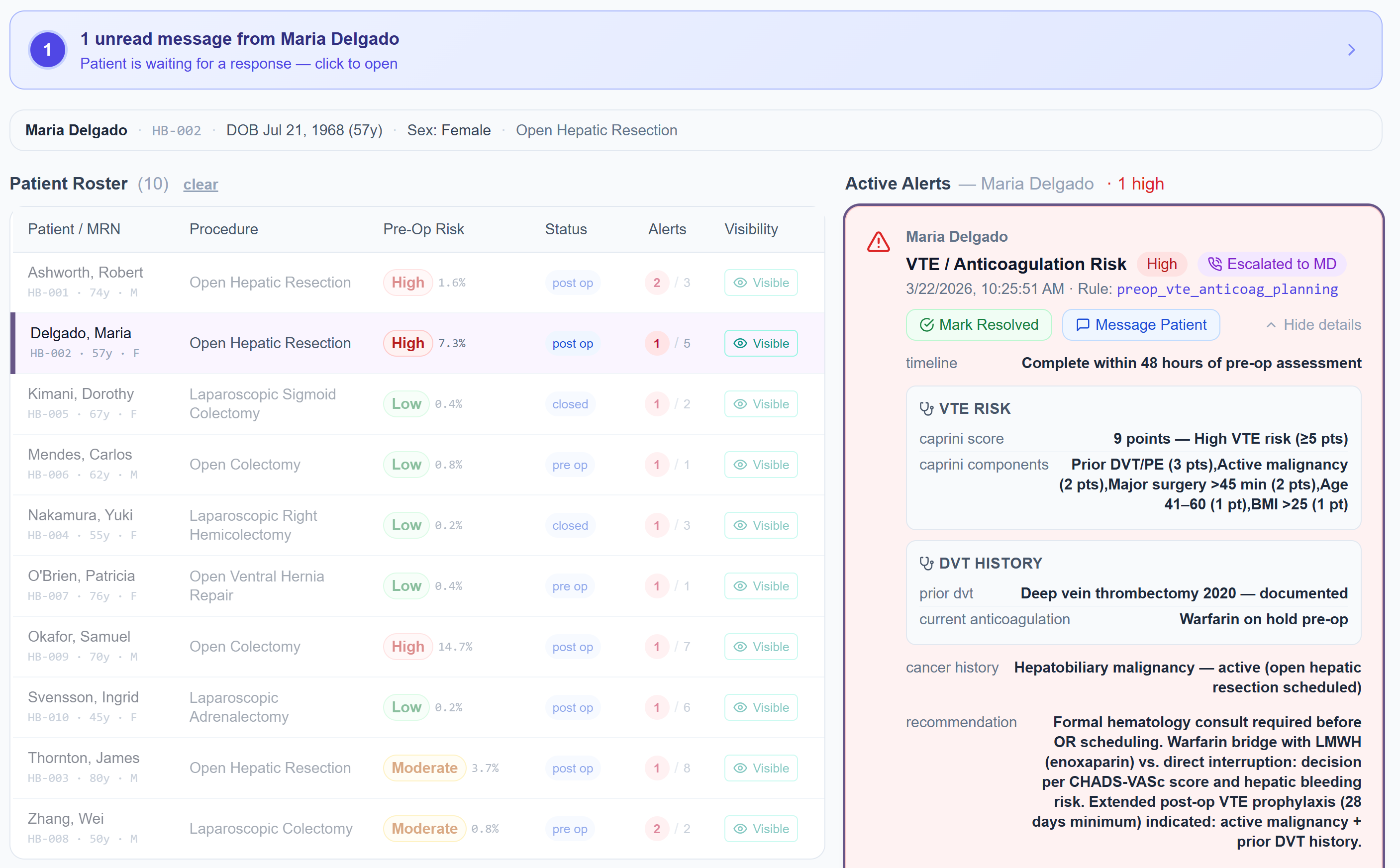
Maria's VTE risk was flagged. Escalated to her MD. Before it became a crisis.
When Maria's Caprini score reached 8 (high VTE risk), combined with a documented history of deep vein thrombosis and an active hepatic malignancy, PeriOptima generated a VTE/Anticoagulation alert and escalated it directly to her attending physician.
The alert doesn't just say "high risk." It includes the full clinical brief: Caprini components, prior DVT documentation, cancer status, and a specific recommendation: formal hematology consultation before OR, with guidance on bridging anticoagulation decisions. The physician has everything needed to act, without hunting through the chart.
Not just a notification. A clinical brief with the context needed to make a decision, delivered to the right provider at the right time.
Patient Engagement
The patient doesn't check out when they check in.
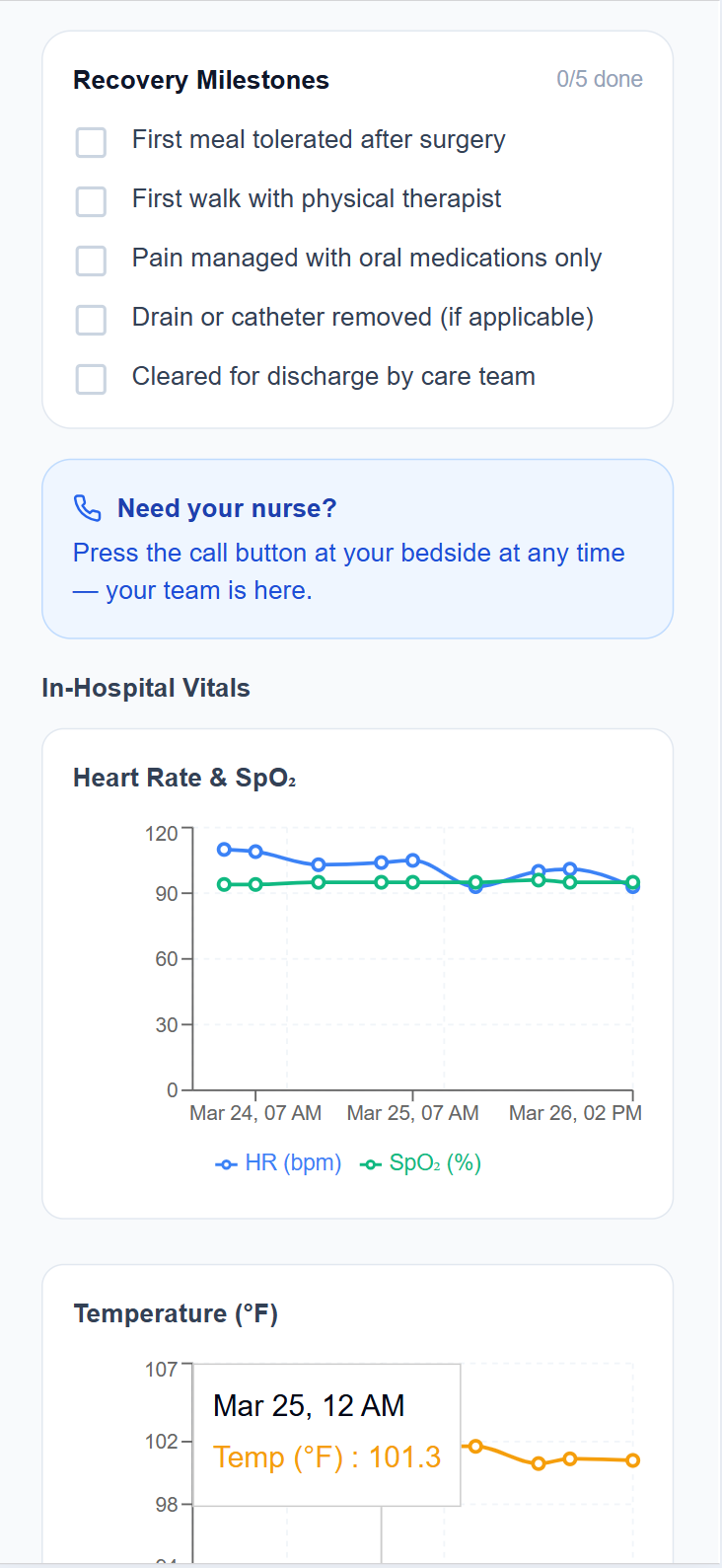
Patients stay connected to their care throughout the inpatient stay. Maria's in-hospital view shows her current EMR vitals, pulled directly from the hospital system via FHIR, alongside her recovery milestones: first meal tolerated, first walk with physical therapist, pain managed on oral medications, cleared for discharge by care team.
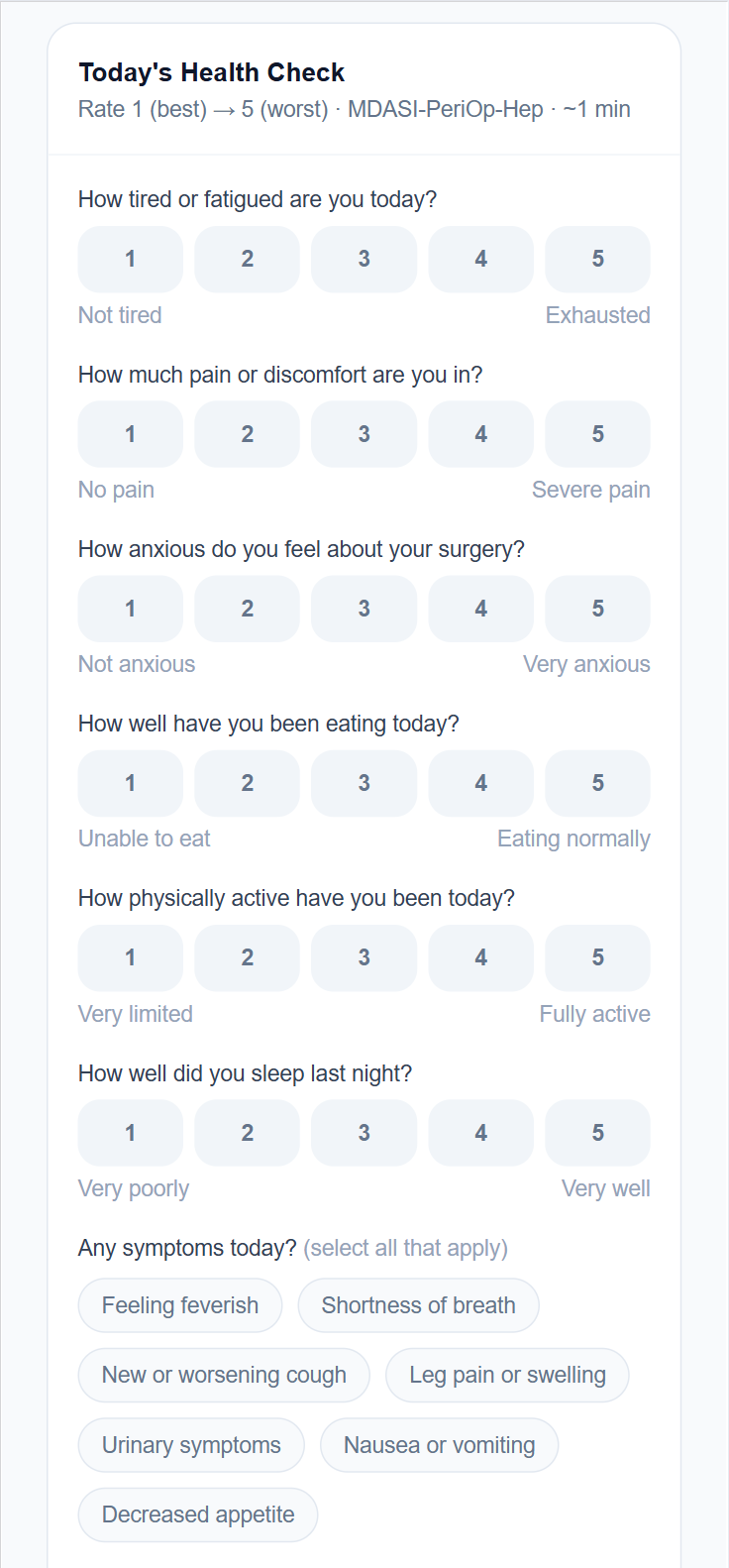
Her daily health check is still active in the hospital: MDASI-PeriOp validated symptom reporting, feeding into the clinical team's view. Every milestone she checks off is visible to her clinical team. Every symptom she reports is logged.
- EMR vitals synced via FHIR (read-only, no workflow changes)
- Procedure-specific recovery milestones visible to patient and team
- Ongoing MDASI-PeriOp check-ins throughout the inpatient stay
- Care team message notifications delivered directly to the app
Home Recovery
Discharge isn't the end — it's the highest-risk window. Complications build slowly, over days, through declining vitals and symptoms patients don't know are warning signs. PeriOptima stays with the patient after the hospital does.
Patient-Reported Outcomes
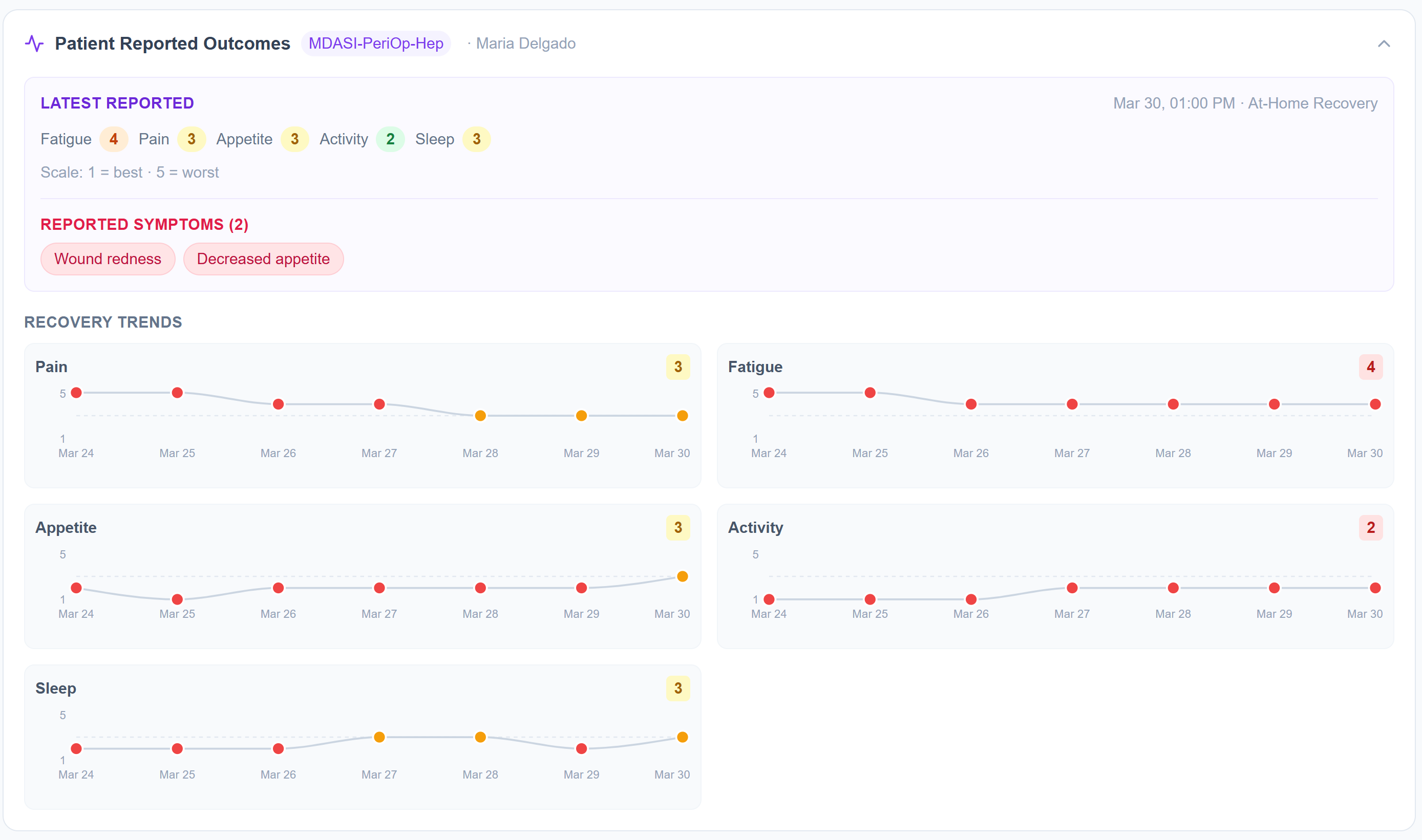
Maria reports. Her team sees the trend.
Every day, Maria rates her pain, fatigue, appetite, activity, and sleep using the MDASI-PeriOp-Hep validated instrument, a peer-reviewed tool designed specifically for perioperative and hepatic populations. The check-in takes about one minute.
Her care team doesn't see a single data point. They see the trend: pain at 3 and rising, fatigue at 4 and flat, appetite declining over five days. A worsening pattern across multiple dimensions is visible before it surfaces as a 2am phone call. Patient-reported outcomes become an early warning system.
- MDASI-PeriOp validated, peer-reviewed, and procedure-specific
- Longitudinal trend view for care team, not just latest scores
- Symptom flags: wound redness, decreased appetite, shortness of breath
- Smart escalation when recovery trends the wrong direction
Remote Monitoring
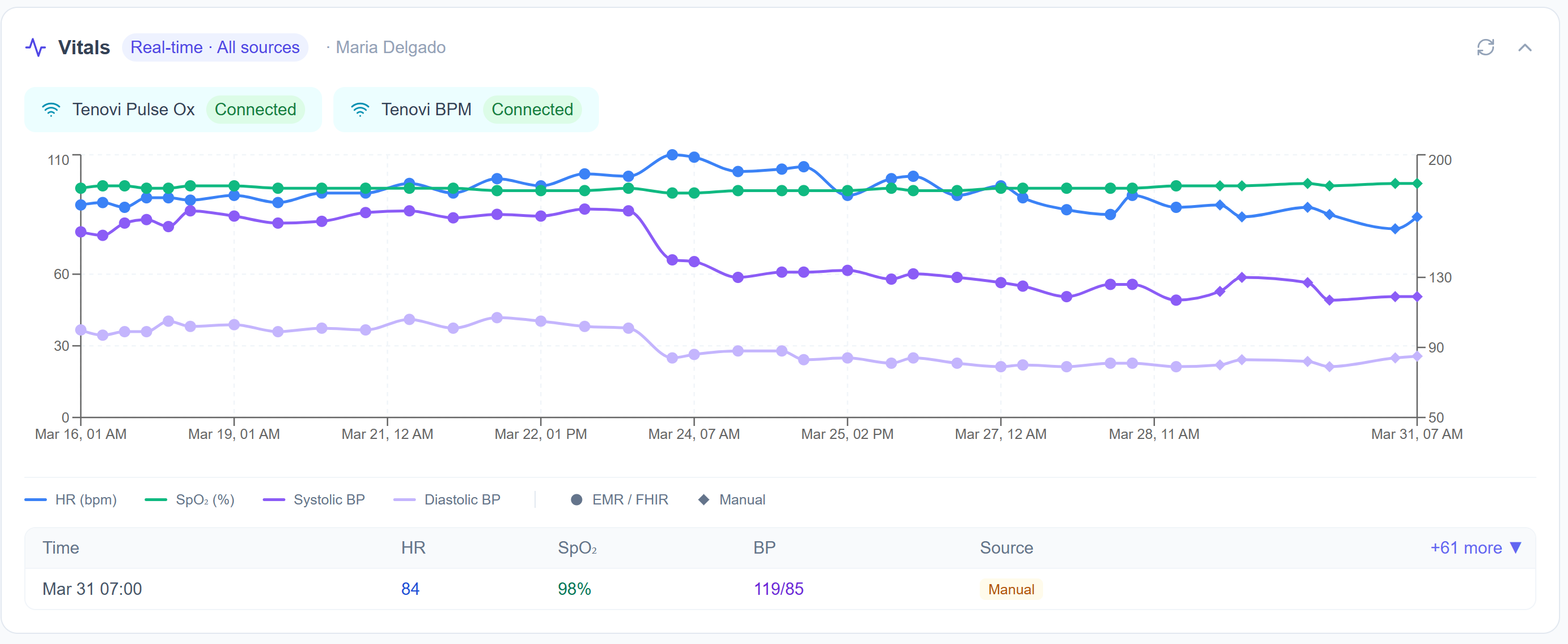
Continuous vitals. Clinician-visible. Without a clinic visit.
Maria's Tenovi Pulse Ox and BPM devices stream vitals directly into her clinical record: HR, SpO₂, and blood pressure, updated continuously throughout home recovery. Clinicians see the full two-week timeline, with each reading labeled by source: FHIR from the hospital EMR, manual entry, or Tenovi device.
The signal is always there, even when Maria doesn't think to report. Declining SpO₂ across three days isn't a phone call waiting to happen. It's a trend that's already visible to her clinical team, with smart escalation thresholds that trigger an alert before it becomes acute.
Compatible with Tenovi RPM devices, Apple HealthKit, and Android Wear OS, on devices patients already own or can be provided before discharge.
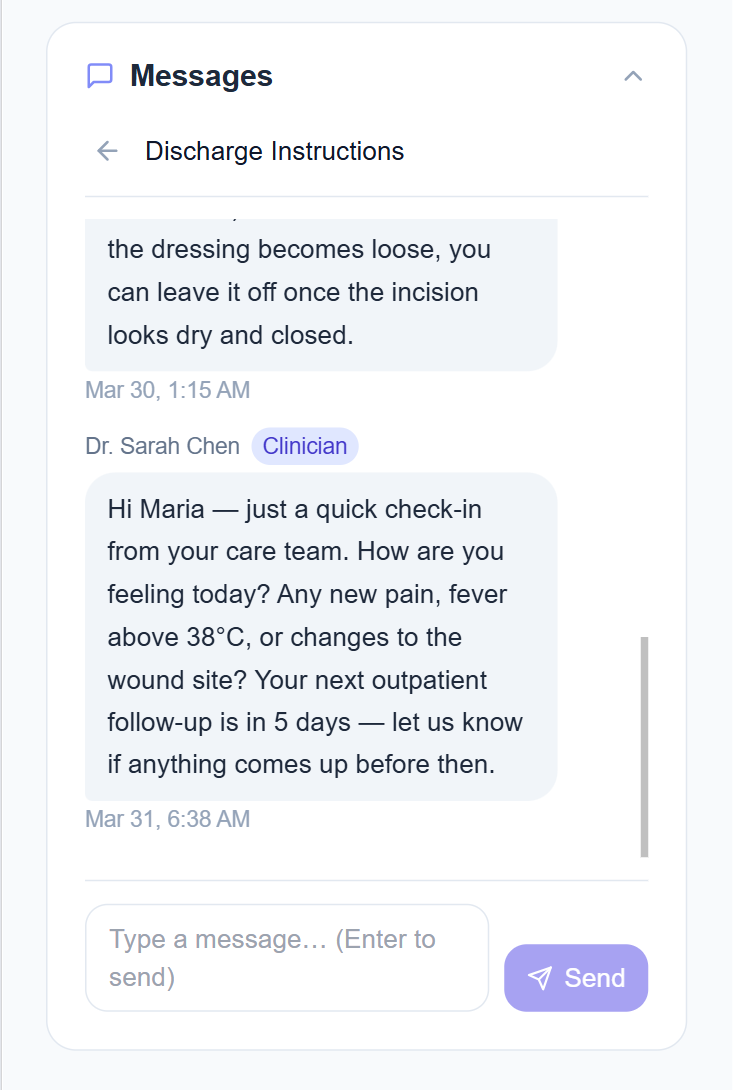
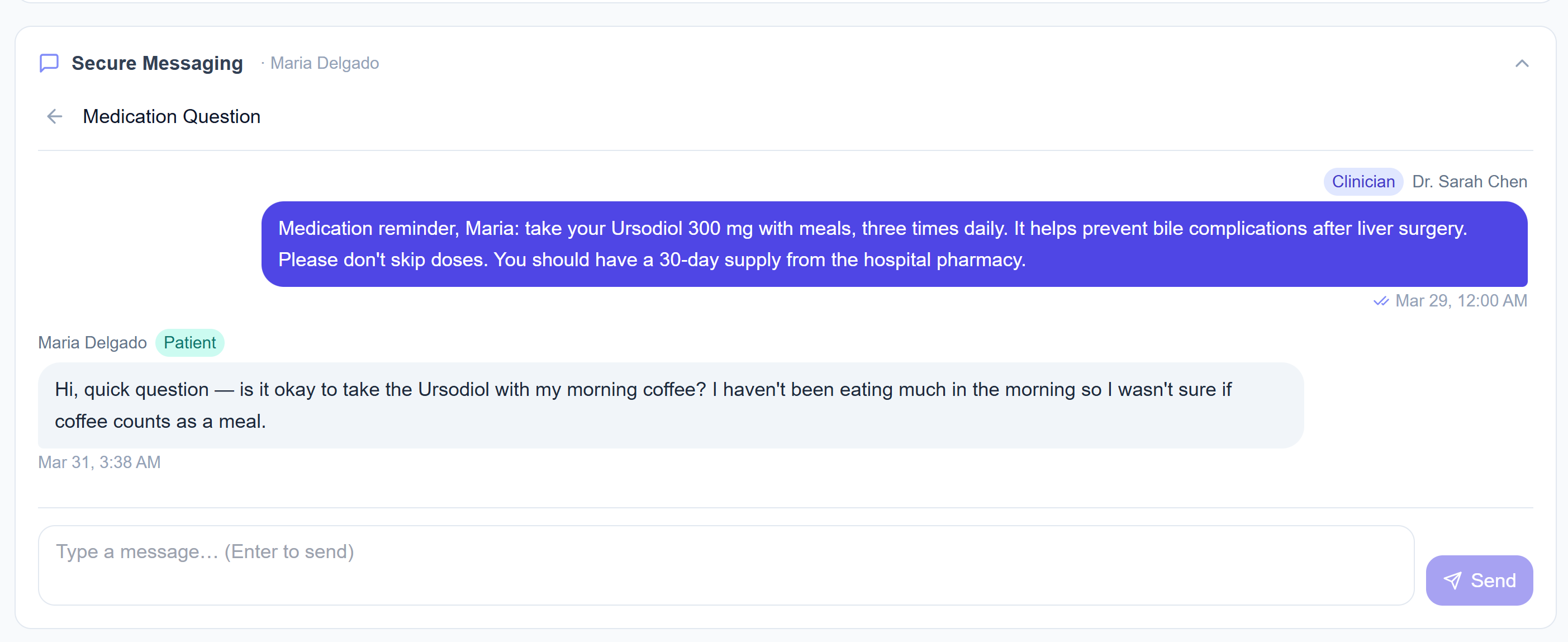
Patient–Clinician Connection
The connection that kept Maria out of the ED.
It was 3:30am when Maria messaged her care team. She was taking Ursodiol after her liver surgery and wasn't sure if coffee counted as a meal. A small question, but the kind that can lead to a skipped dose, a complication, or an unnecessary ED visit.
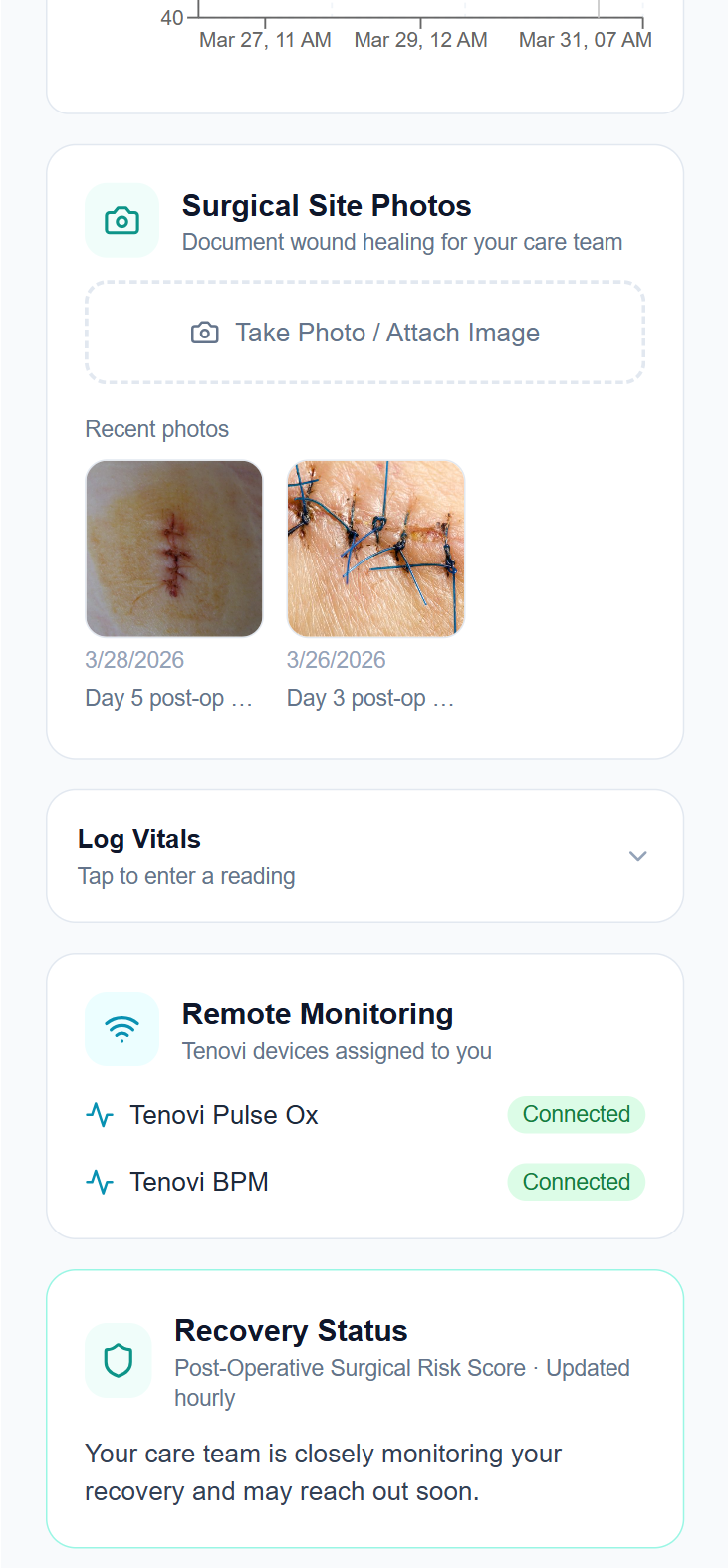
Wound Monitoring
Wound photos. Vitals. Recovery status. In one place.
Maria's home recovery dashboard brings together everything her care team needs to monitor her at a distance. She photographs her surgical site from her phone, reviewed by her care team, not just filed. Her Tenovi devices show as connected and actively streaming. Her post-operative surgical risk score is updated automatically as her recovery data accumulates.
Routine follow-up is handled through the app. Her care team is notified when something needs attention, not because they're monitoring constantly, but because PeriOptima is.
- Wound photo uploads with date and care team annotations
- Tenovi remote monitoring device status and connection health
- Post-operative surgical risk score, updated continuously
- Smart escalation: clinical team notified only when needed
Recovery Guidance
ERAS-based recovery guidance. In the patient's pocket.
Maria's recovery guide is built on ERAS® Society 2022 guidelines, personalized to her procedure. Walking from day one. Return to normal eating. Hydration and bowel function. Opioid-sparing pain management. Daily wound monitoring. All of it in plain language, not clinical instructions designed to be filed away.
An AI recovery assistant is available around the clock to answer questions about wound care, diet, activity, and symptoms, providing consistent, evidence-based guidance that reduces unnecessary calls to the clinic without leaving patients without answers.
Routine follow-up is automated. Clinical staff intervene only when a patient needs them, not to answer every question about what to eat or when to shower.
See It In Action
Ready to see PeriOptima in your system?
We're working with a small number of health systems in a structured 90-day pilot: 50–100 patients, read-only Epic integration via FHIR, zero workflow disruption. No procurement process required to start the conversation.